Disasters cause widespread flooding and property damage that expose employees to hazards during cleanup and recovery. Employers sending employees into Disaster Cleanup Area’s to do recovery have a responsibility, according to OSHA, to train employees appropriately and provide personal protective equipment.
Contaminated Floodwaters
The mold and fungi in the air employees breathe have the potential to make them sick. Bacteria and other infectious organisms (from sewage) in water and soil as well as toxic substances from flooded industrial and waste sites pose big hazards.
-
- Employers must ventilate enclosed spaces with fresh air.
- Assume that floodwater is contaminated unless proven otherwise.
- Allow only trained workers with the proper personal protective equipment to clean up toxic chemicals, other hazardous waste, and mold.
- Employees must be up-to-date with a tetanus shot (within the last 10 years).
- Discarding water-damaged and visibly contaminated materials while wearing waterproof boots, latex or rubber gloves and other protective clothing.
- Employers must consider using special chemical-resistant outer clothing and protective goggles in some cases depending on the hazard.
- Issue N-95 NIOSH-approved disposable respirator, at a minimum, when handling mold-contaminated materials and this respirator requires medical evaluations and fit test prior to use.
- Employers must keep an adequate supply of clean water available for drinking and washing.
Downed Power Lines
Burns and electrocution from contact with energized lines or objects, including tree limbs, in contact with downed power lines.
-
- Establish and clearly mark a danger zone around all downed power lines
- Stay at least 10 feet from all downed lines
- Assume that all power lines are live or energized
- Allow only trained and equipped workers to repair electrical wires
Tree Trimming and Debris Removal
Electrocution is not the only hazard as being struck or crushed by falling trees and limbs can cause severe injury or death.
Employers must:
-
- Contact utility companies and request they de-energize and ground or shield power lines.
- Require all tree trimming and removal with 10 feet of a power line must be performed by trained tree trimmers
- Establish and clearly mark danger zones where tree debris may fall onto workers
- Protect employees from injuries from equipment from lifting or moving tree limbs and other debris
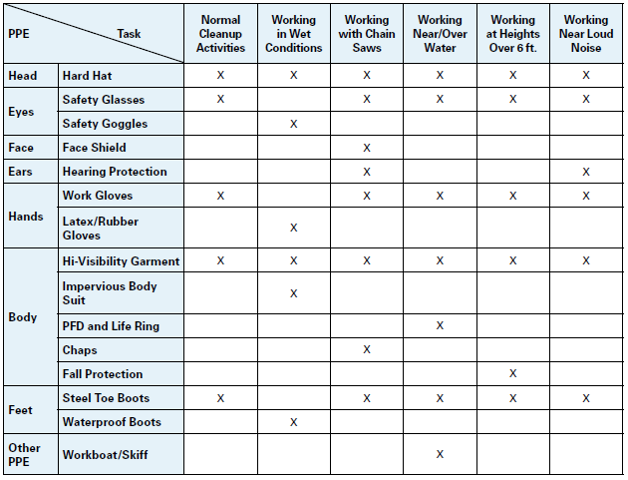
- Provide employees with work personal protective equipment (PPE) such as gloves, hard hats, boots, hearing protection and eye/face protection. Chaps should be provided when using a chainsaw.
- Train Employees on chainsaw’s require employees to watch for kickback and not cutting with the saw tip
- Training on not getting to close to chippers as well as, not reaching into a chipper
- Provide mechanical equipment to lift heavy objects or provide extra people and training in proper lifting techniques
Falls
Falls from aerial lifts, ladders, roofs and other elevated work surfaces can be hazards for employees. Slippery and uneven working surfaces that can create injuries due to slips.
Employers must provide the following protective measures:
-
- Use safe procedures to prevent aerial lift tip-overs
- Provide employees with body harness or restraint belt with a lanyard attached to the boom or basket of the lift
- Use proper ladder safety (set on firm and stable ground, maintain “three-point” contact, do not stand on top rung)
- Be aware of wet or slippery surfaces, obstacles, or uneven surfaces on the site
Portable Generators
Shocks and electrocution from gas and diesel powered generators, as well as toxic carbon monoxide (CO) from generator exhaust are hazards as disaster recovery sites. Fires from improper refueling and fuel storage are also problems.
Employers must:
-
- Never run a portable generator inside a house or enclosed space
- Inspect electric cords to ensure they are in good working condition and free of any defects
- Use a ground-fault circuit interrupter (GFCI)
- Ensure that spaces where generators are used are properly ventilated
- Shut down the generator before refueling
- Never store fuel or the generators indoors
Work Zones
Transportation incidents (injuries and deaths) in work zones where workers are struck by moving vehicles and mobile equipment.
Employers must use the following preventive measures:
-
- Wear high-visibility clothing and headwear compliant with ANSI/ISEA 107-2004
- Use proper traffic controls (Signs, cons, barriers)
- Use proper lighting, flaggers, and worksite communications
- Make sure that vehicle operators are properly trained
- Always use seat belts and rollover protection
Construction Activities
Exposure to asbestos contaminated materials during the demolition of building and structures has a high probability at disaster sites. Spaces with limited access, suffocation hazards, or confined spaces can be confronted. Employees can be exposed to trenching and excavation accidents such as cave-ins. An employee is at risk for back, knee and shoulder injuries from manual lifting and handling of building materials and fallen trees.
Employers must:
-
- Properly select and require the use of PPE which may include respiratory protection
- Do not allow employees to enter permit-required confined spaces with training an a permit to enter
- Prevent cave-ins by benching, sloping, shoring, or shielding the soil
- Require the use of proper lifting techniques and teams of two or more to move bulky or heavy items